delta dental appeal form
DeltaCare Specialty Referral Form Use this form to refer your patient to a specialist. Optional Treatment Consent Form Use this form if your patient elects to have optional treatment completed.

Sample Letters Of Appeal To Dental Insurance Lovetoknow
Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.

. However when special circumstances arise Delta Dental of Kansas may require additional time to reach a final decision. Delta Dental of Michigan is a part of Delta Dental Plans Association. Skip Navigation This page features a timed image rotator.
Theres no hassle in working through claims saving you time and frustration. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US. Use this secure form to file a grievance or appeal a dental benefits decision.
Delta Dental of Minnesota provides free aids and services to people with disabilities to communicate effectively with us such as. Director Professional Relations Northeast Delta Dental One Delta Drive PO Box 2002 Concord NH 03302-2002. Automatic bank draft authorization for risk groups.
CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX. The Appeal Request Form must be received by Delta Dental of Kansas within 180 calendar days from the date of the original adverse benefit determination or the corresponding remittance advice. Complaint and appeal form Section 2.
The information provided on this site is for general education purposes only and is not intended as a diagnosis treatment or a substitute for professional medical or dental advice diagnosis or treatment. Box 40384 Portland OR 97240 or fax to 503-412-4003 or 866-923-0412. A claim review for resubmission can be completed by Delta Dental in.
NPI National Provider Identifier Identity TheftProtect Your Practice from Patient Fraud. The law requires the following be placed on all plan grievance forms. THE PO BOX IS FOR CLAIMS ONLY.
Oral Health Services for Children Adolescents with Specials Health Care Needs. Delta Dental of California. Locum Tenens Provider Form.
Delta Dental HIPAA Form 14b ASO Groups. We cover more Americans than any other dental benefits provider - and strive to make dental coverage more accessible and affordable to a wide variety of employers groups and individuals. Attach additional pages if needed.
Qualified sign language interpreters Written information in other formats. Dental plans provided by Oregon Dental Service ODS dba Delta Dental Plan of Oregon and Delta Dental of Alaska. Dentist Administrative and Authorization Forms.
This site is meant to. Delta Dental of Ohio is a part of Delta Dental Plans Association. View additional forms by logging in to your secure member portal.
Appeal Form - Information on how to appeal your claim. Mail this form to Delta Dental. Through our national network of Delta Dental companies we offer dental coverage in all 50 states Puerto Rico and other US.
Questions about the appeals process you may call the Departments Consumer Assistance Office at 602 3642499 or 8003252548. Delta Dental PPO participation packet request. Your appeal or if necessary request additional information regarding your appeal within 20 business days of receipt.
Delta Dental of Oregon is a part of Delta Dental Plans Association. We cover more Americans than any other dental benefits provider - and strive to make dental coverage more accessible and affordable to a wide variety of employers groups and individuals. If you would like to disable it press enter now.
Group Information Change Request Form. Through our national network of Delta Dental companies we offer dental coverage in. Healthy Smile Healthy You enrollment form Spanish.
After receiving this Appeal Request Delta Dental of Kansas will either send you a written decision regarding your appeal or if necessary request. Complaint or appeal Please write your complaint or appeal in the space below and on the back of this page. Find solutions that make it easier to manage your practice like benefit information and claims status.
CLAIMS APPEALS SENT TO THE PO BOX WILL BE DELAYED. Delta Dental of Minnesota does not exclude people or treat them differently because of race color national origin age disability or sex. Delta Dental HIPAA Form 14a Risk Groups.
To submit an appeal complete the Form in its entirety and attach all documents records and any. Delta Dental is Americas largest and most trusted dental benefits carrier. DeltaCare USA participation packet request.
This form is not needed for orthodontic referrals. Dental Office Support Resources. You will receive a written decision on your request for review within 30 days unless more information.
With Delta Dental we keep you smiling. Dental Office Toolkit - User Guide. You will receive written confirmation of your grievance within 5 days.
Please refer to the vision appeals packet for information on submitting DeltaVision Administered by EyeMed appeals. Reconsiderationappeal requests must be submitted within six 6 months of the date of the original explanation of benefitspayment remittance advice. Dentists should submit their reconsiderationappeal request to.
Delta Dental Premier Network Forms - Professional Application Credentialing form Delta Dental Premier Dentists Agreement Ownership Control Form and W-9. Delta Dental is Americas largest and most trusted dental benefits carrier. Continuous Orthodontic Coverage Form.
ASO contract addendum for HIPAA privacy and security. Through our national network of Delta Dental companies we offer dental coverage in. Use this form to update the status of your practice as a DeltaCare provider.
How to Know When You Can Appeal When Delta Dental does not authorize or approve a service or pay for a claim we must notify you of your right to appeal that decision. Delta Dental requires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical corrections or to provide additional information to support the original claim submitted. Healthy Smile Healthy You enrollment form.
2
2
2
2
2
2
2
2
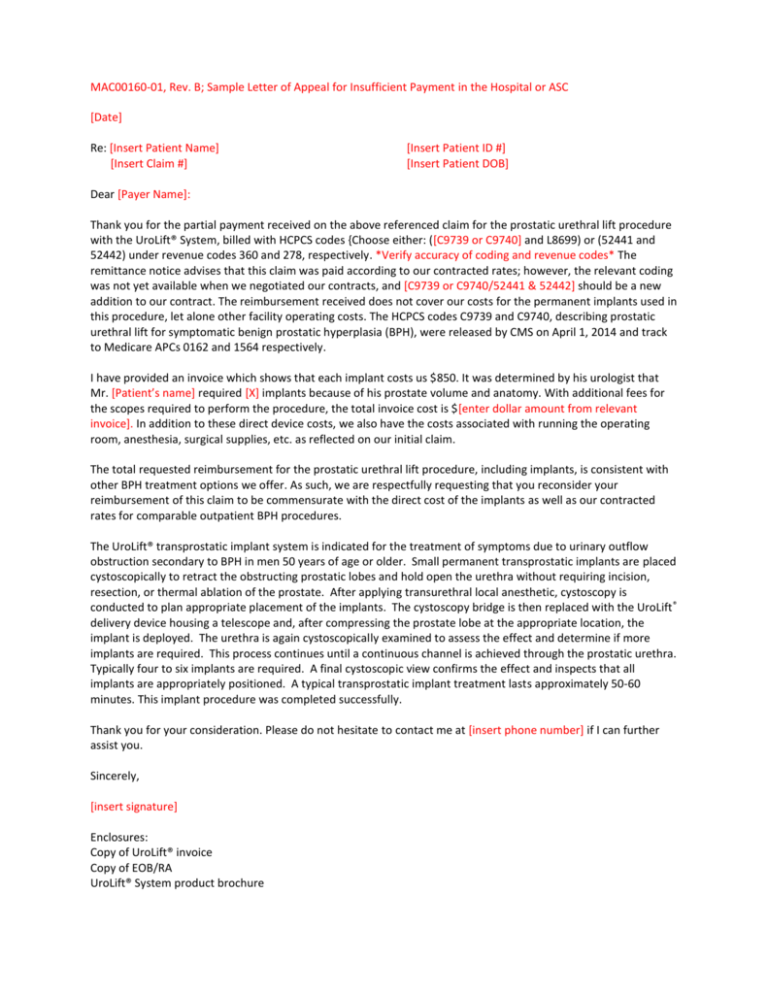
Sample Letter Of Appeal For Insufficient Payment Hospital
2
2
2

News Release Delta Dental Of Wisconsin
2
2
2

Fillable Online Disabled Dependent Application Delta Dental Massachusetts Form Fax Email Print Pdffiller

Sample Letters Of Appeal To Dental Insurance Lovetoknow
Claim And Admin Forms Delta Dental